
Designing with Care: Why Fidelity, Flexibility and Psychological Safety Matter in Parenting Support
By Rachel A.Wood. The inspiration for this blog came from reflecting on the second study in my research. It reflects on what it means to design parenting support with care, emphasising that services are shaped not only by their evidence base, but by how safe, flexible, and supportive they feel to parents. Bringing together insights from trauma theory, developmental psychology, implementation science, and design psychology, it explores how fidelity, flexibility, and psychological safety work together in practice. The blog invites us to consider how everyday design choices can quietly support, or unintentionally undermine parents’ engagement, agency, and trust.
When we talk about trauma-informed parenting support, it’s easy to focus on what a service delivers. But just as important is how parents experience support. As trauma, adversity, and chronic stress are increasingly recognised as shaping parents’ engagement with support, it has become clear that evidence‑based content alone can be insufficient. Designing with care in parenting services means intentionally balancing fidelity to core evidence‑based and trauma‑informed principles, flexibility in responding to diverse contexts and lived experiences, and the creation of psychological safety as a prerequisite for engagement and learning. This blog draws together insights from trauma theory, developmental psychology, implementation science, and design psychology to explore how these three interdependent principles can be held in tension, and how design choices at every level of service delivery can either support or undermine parents’ sense of safety, agency, and trust.
In this context, designing with care refers to intentionally shaping services in ways that prioritise safety, dignity, and agency, recognising that design choices are never neutral, and always communicate values, particularly for parents with experiences of trauma or adversity.
In plain terms trauma informed practice starts from the assumption that people’s past experiences shape how safe, trusting, or in control they feel now, especially in services that involve judgement, authority, or personal disclosure.
At its core, trauma-informed practice is grounded in an understanding of how trauma affects neurological, emotional, and relational functioning. Foundational work highlights that trauma disrupts an individual’s sense of safety, trust, and control, often leading to heightened threat perception and difficulties with emotional regulation (Herman, 1992). These insights have been translated into widely adopted principles, including safety, trustworthiness, choice, collaboration, and empowerment (SAMHSA, 2014). Within parenting contexts, this translates into recognising that behaviours often labelled as ‘resistant’ or ‘disengaged’ may instead reflect adaptive responses to perceived threat or prior relational harm.
Put simply attachment theory helps explain how early relationships shape our expectations of others, including whether we expect support to feel safe, responsive or rejected.
To understand why this matters, it helps to briefly revisit what trauma-informed practice is grounded in. Attachment theory provides a complementary foundation for trauma-informed parenting support. Early relationships shape children’s internal working models of safety and connection, with sensitive and responsive caregiving supporting secure attachment and emotional regulation (Bowlby, 1969; Ainsworth et al., 1978). However, parents who have experienced trauma may themselves struggle with regulation and relational trust, potentially impacting their capacity to provide consistent caregiving. This underscores the importance of parenting support that does not simply teach skills, but actively support co-regulation, reflection, and relational repair.
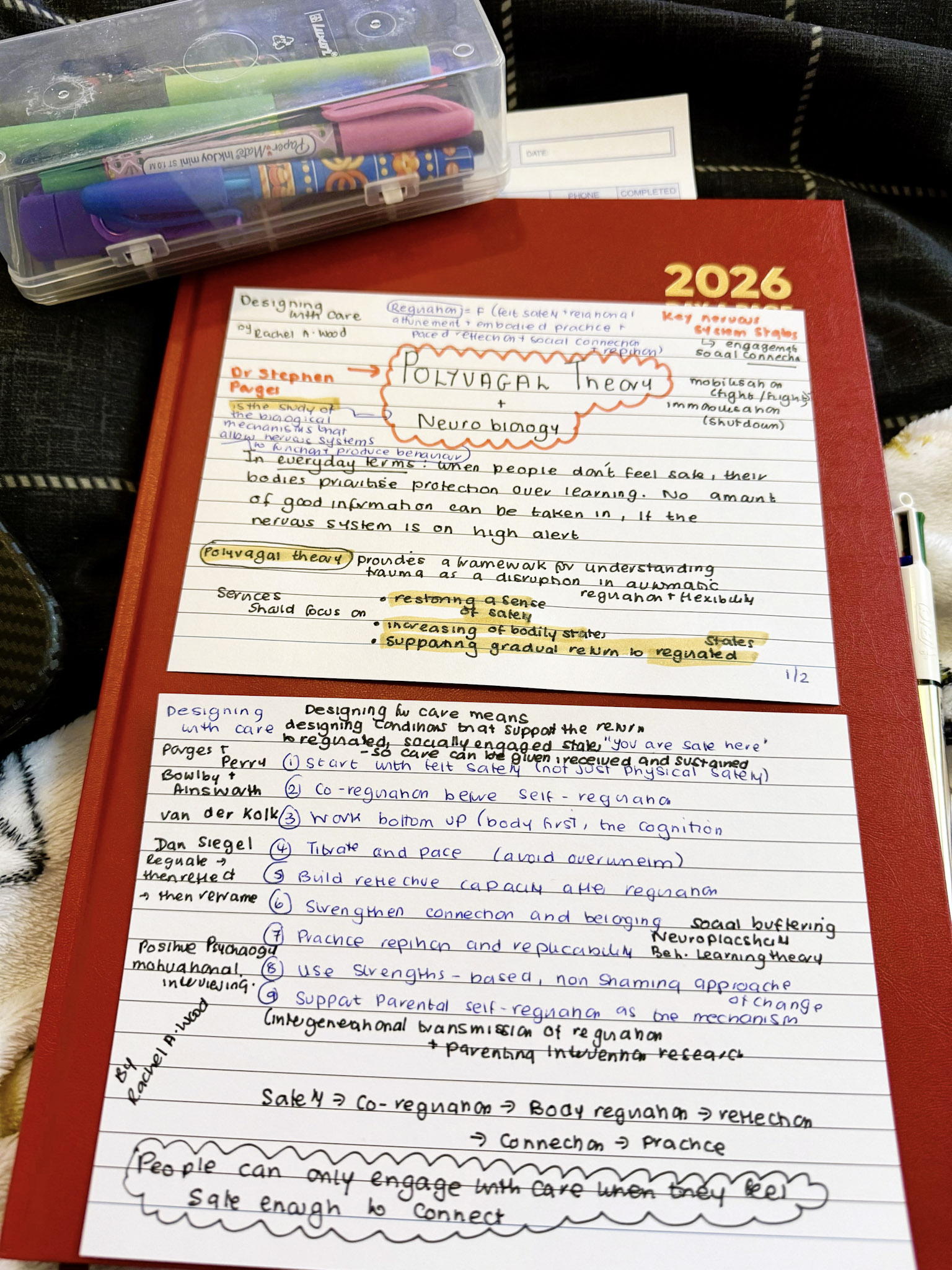
From a neurobiological perspective, polyvagal theory further illuminates the importance of safety in shaping behaviour. It suggests that individuals continuously and unconsciously scan for cues of safety or threat, with physiological states influencing their capacity for social engagement and learning (Porges, 2011). In practice, this means that parenting services must attend not only to content, but to the emotional and sensory environment in which learning takes place. Without a sense of safety, parents are unlikely to engage meaningfully with new ideas or strategies.
The concept of psychological safety, originally developed within organisational research, is particularly relevant here. Psychological safety refers to the shared belief that it is safe to take interpersonal risks, such as admitting difficulties or asking for help, without fear of judgement or negative consequences (Edmondson, 1999). In parenting support, where shame and fear of judgement are often pronounced, psychological safety becomes a prerequisite for engagement, not a ‘nice to have’ but a foundational condition. Studies consistently show that non-judgemental, empathetic practitioner relationships are central to sustained participation and positive outcomes in parenting programmes (Axford et al., 2012).
This is where a familiar tension emerges for many practitioners (including myself): how closely should services be delivered as designed, and where is adaptation necessary?
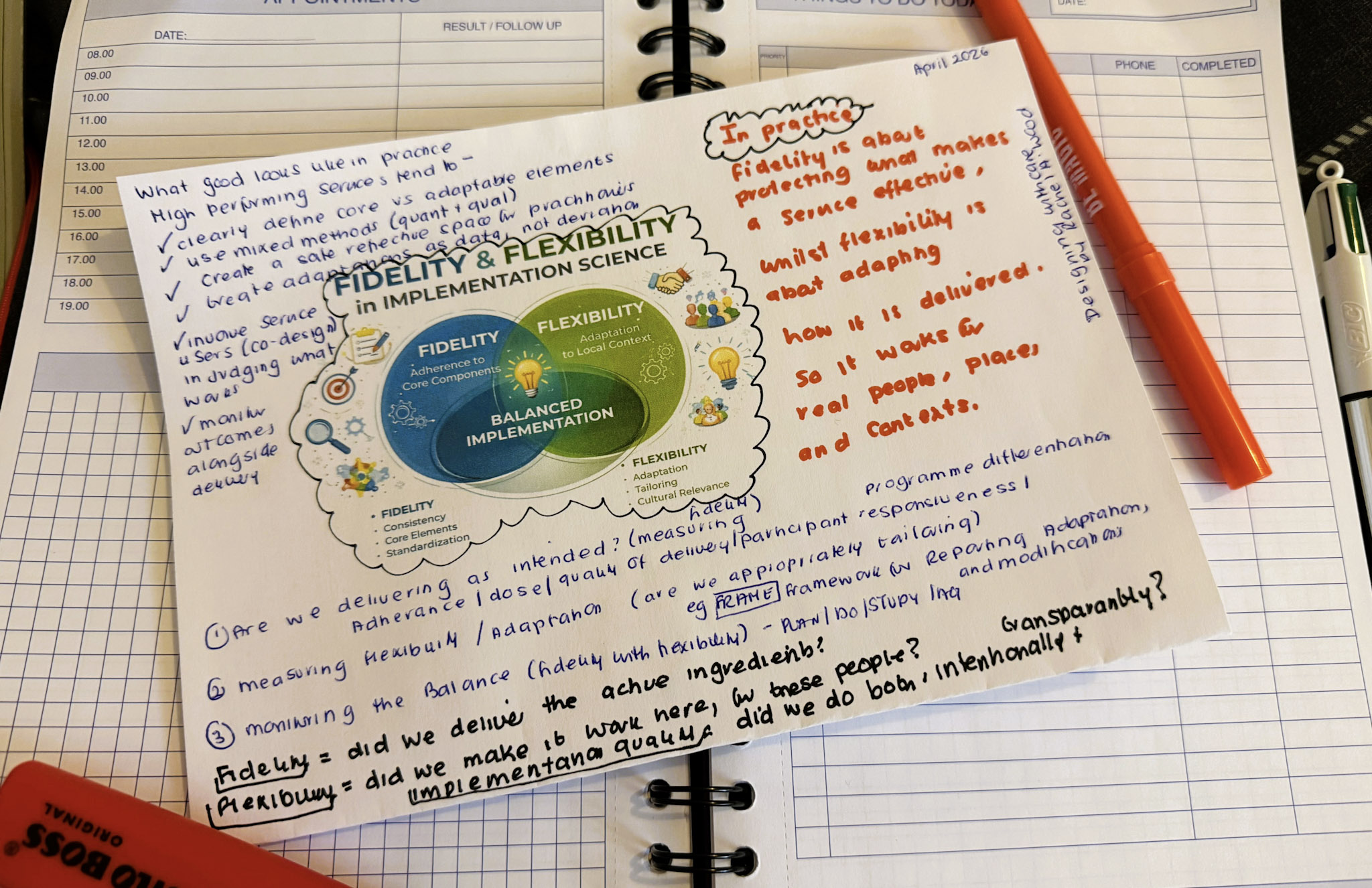
Alongside these relational and emotional considerations, implementation science provides important insights into how evidence-based programmes are delivered in practice. A key tension identified in the literature is that between fidelity and flexibility. Fidelity refers to the degree to which a programme is delivered as intended, which is associated with improved outcomes (Fixsen et al., 2005). However, strict adherence without adaptation can reduce relevance and accessibility, particularly for diverse or marginalised populations (such as in my research). Conversely, excessive adaptation may dilute the core components that make interventions effective. Emerging consensus suggests that effective implementation involves maintaining fidelity to core principles while allowing flexibility in delivery, often described as adaptive fidelity (Moore et al., 2013).
In trauma-informed parenting support, this balance is particularly critical.
Fidelity must extend beyond service content to include adherence to trauma-informed principles such as safety and empowerment. At the same time, flexibility is essential to accommodate diverse trauma experiences, cultural contexts, and varying
levels of readiness for engagement. This aligns with ecological systems theory, which emphasises that parenting is shaped by multiple interacting systems, including family, community, and wider socio-economic conditions (Bronfenbrenner, 1979). From a care perspective, this balance is not simply technical. Decisions about fidelity and flexibility shape whether parents feel contained or constrained, supported, or scrutinised.
In trauma‑informed contexts, care is not only expressed through relationships, but through the design of systems, processes, and environments themselves. Design psychology offers a valuable lens for understanding what it means to design with care in practice. Rooted in human-centred design and behavioural science, it focuses on how environments, systems, and interactions influence human behaviour and experience (Norman, 2013). From this perspective, parenting support is not simply a set of sessions, but a series of designed experiences, from the first referral conversation to the room a group meets in. This importantly needs to include implicit messages about safety, power, and belonging. For example, unclear referral processes, inconsistent communication, or overly formal environments may inadvertently signal threat or judgement, undermining engagement.
Design Psychology focuses on how services, systems, environments, and interactions influence how people think, feel and behave (often without realising).
Key principles from design psychology, such as reducing cognitive load, enhancing predictability, and supporting beneficiary agency, are highly relevant in trauma-informed contexts. Cognitive load theory suggests that individuals may have limited capacity for processing information, which is further reduced under stress (Sweller, 1988). Parenting services that are overly complex or information-heavy may therefore be less effective for parents experiencing trauma. Predictable structures and clear communication help reduce uncertainty.
In plain terms cognitive load theory is when people are stressed or overwhelmed, their capacity to absorb new information is reduced.
The concept of choice architecture also intersects with trauma-informed principles. Providing meaningful choices within services can enhance a sense of control and autonomy, counteracting the loss of agency often associated with trauma (Thaler and Sunstein, 2008). In practice, this may involve offering different modes of participation, allowing parents to set goals collaboratively, or providing options for how and when to engage.
Choice architecture: In everyday terms the way choices are presented can either support people to feel in control or leave them feeling pressured or powerless.
A number of high-quality practice frameworks bring these theoretical insights together. The SAMHSA (2014) trauma-informed care framework remains a cornerstone, widely adopted across health and social care systems. The Adverse Childhood Experiences (ACEs) framework has also been influential in highlighting the long-term impact of early adversity on health and behaviour (Felitti et al., 1998). In the UK context, trauma-informed approaches are increasingly embedded within early help and family support strategies, often alongside strengths-based and restorative practice models.
Reflective practice and systems: Trauma informed practice is not just about individual skills. It depends on organisational cultures that support reflection, supervision, and emotional safety for as well.
Reflective practice frameworks are also central, recognising that practitioners’ ability to provide trauma-informed support depends on their own emotional awareness and regulation. Regular supervision and opportunities for reflection are therefore considered essential components of trauma-informed systems (Ruch, 2007). This aligns with the broader systems perspective that trauma-informed practice is not solely an individual competency, but an organisational and cultural approach.
In putting together this blog, it becomes really clear that trauma-informed parenting support is most effective when it is intentionally designed across multiple levels. It requires fidelity to evidence-based and trauma-informed principles, flexibility to adapt to diverse contexts, and a consistent focus on psychological safety. Design psychology provides a unifying framework for understanding how these elements are experienced by parents, emphasising that every interaction and environment shapes engagement and outcomes.
Ultimately, designing with care in trauma‑informed parenting support involves a shift from simply delivering services, to intentionally shaping experiences. It requires fidelity to the core evidence‑based and trauma‑informed principles that underpin effectiveness, flexibility in how these principles are enacted across diverse contexts and lived experiences, and a sustained commitment to psychological safety as the foundation for engagement, learning, and change. Trauma-informed parenting support is therefore not only about what is taught, but about how parents experience the service, whether interactions feel safe, respectful, and empowering in practice, not just in principle. When these conditions are designed for and consistently upheld, parents are more likely to engage meaningfully, reflect on their experiences, and make changes that support both their own wellbeing and that of their children.
Designing with care, then, involves more than delivering well‑evidenced services. It requires ongoing attention to how services are experienced, and a commitment to shaping conditions that support safety, agency, and trust over time.
References
Ainsworth, M.D.S., Blehar, M.C., Waters, E., and Wall, S. (1978) Patterns of attachment: A psychological study of the strange situation. Hillsdale, NJ: Erlbaum.
Axford, N., Lehtonen, M., Kaoukji, D., Tobin, K., and Berry, V. (2012) ‘Engaging parents in parenting programs: Lessons from research and practice’, Children and Youth Services Review, 34(10), pp. 2061–2071.
Bowlby, J. (1969) Attachment and loss: Vol. 1. Attachment. London: Penguin.
Bronfenbrenner, U. (1979) The ecology of human development. Cambridge, MA: Harvard University Press.
Edmondson, A. (1999) ‘Psychological safety and learning behavior in work teams’, Administrative Science Quarterly, 44(2), pp. 350–383.
Felitti, V.J., Anda, R.F., Nordenberg, D., Williamson, D.F., Spitz, A.M., Edwards, V., Koss, M.P. and Marks, J.S. (1998) ‘Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults’, American Journal of Preventive Medicine, 14(4), pp. 245–258.
Fixsen, D.L., Naoom, S.F., Blase, K.A., Friedman, R.M. and Wallace, F. (2005) Implementation research: A synthesis of the literature. Tampa, FL: University of South Florida.
Herman, J.L. (1992) Trauma and recovery. New York: Basic Books.
Moore, G.F., Audrey, S., Barker, M., Bond, L., Bonell, C., Hardeman, W., Moore, L., O’Cathain, A., Tinati, T., Wight, D., and Baird, J. (2013) ‘Process evaluation of complex interventions’, BMJ, 350, h1258.
Norman, D.A. (2013) The design of everyday things (Revised edn). New York: Basic Books.
Porges, S.W. (2011) The polyvagal theory. New York: Norton.
Ruch, G. (2007) ‘Reflective practice in contemporary child-care social work’, British Journal of Social Work, 37(4), pp. 659–680.
SAMHSA (2014) SAMHSA’s concept of trauma and guidance for a trauma-informed approach. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Sweller, J. (1988) ‘Cognitive load during problem solving’, Cognitive Science, 12(2), pp. 257–285.
Thaler, R.H. and Sunstein, C.R. (2008) Nudge: Improving decisions about health, wealth, and happiness. New Haven, CT: Yale University Press.
Leave a Reply